A Case Report of Posterior Open Bite Caused by Using Aligner
~アライナー治療により生じた臼歯部開咬合の一症例~
Hoshi Takao 星 隆夫(神奈川県 相模原市 星歯科矯正)
Ⅰ.Introduction
In recent years, the movement of teeth by aligners has become popular.
Clearliner, Invisaline or similar products are supplied. In the Invisaline it is possible to make all the necessary mouthpieces for treatment from a single impression before treatment. There are also products that make impressions every time a mouthpiece is manufactured.
The Invisaline started to be used in Europe and U.S. in the latter half of the 1990s and was introduced in Japan in 2005. After that, various papers were published on its therapeutic effect. Most of them were case reports. There were relatively few systematic reviews 1) and case control studies 2). A systematic review published in 2017 included three prospective cohort studies and one RCT. The treatment duration and outcomes (Occlusal index scores) and post-treatment stability of fixed appliances and Invisaline are discussed. The results show that the fixed appliance has a longer treatment period and chair time.Occlusal index scores are 13 points lower, and patients with Invisaline are not cured. Post-retention changes were greater in patients with Invisaline.However, Number of papers included are small and the number of cases is inadequate. Therefore, this systematic review is considered unreliable. There is a retrospective case control study that examined many cases. 1,500 Fixed appliance cases, 250 Invisaline cases were examined. 62 and 61 patients respectively was chosen. From those,cases judged not to be treated properly were excluded. 48 patients were selected in each group. The selected patients were 16 years old or above and were treated without tooth extraction. Peer assessment rating index of fixed appliance before treatment is 22.79. The Peer assessment rating index before treatment for Invisaline was 20.81. There was no significant difference. After treatment PAR improved 30% in both groups.There was no significant difference between the two groups. However, statistical analysis showed that the fixed appliance significantly reduced PAR. There was great variability in PAR at the end of Invisaline treatment.It was shown that there were large variations in the finishing of the treatment in Invisaline patients. Invisaline treatment was 5.7 months shorter than fixed appliance treatment. Those were the results. Cases judged to have not been adequately treated were excluded. It is undeniable that the judgment criteria may be a big bias in this paper. Summarizing these results.In non-extraction treatment, treatment period is shorter with Invisaline but the treatment results are inferior to the treatment results when using fixed appliances. On the other hand, cases with inadequate treatment outcomes were excluded from the results. What were the excluded cases? If they are included, the post-treatment PAR index how does the index change?
Orthodontic treatment is a medical treatment that creates a proper occlusion of the upper and lower teeth. In aligner treatment, the teeth do not move if the aligner is not attached. With the aligner attached, if prevents the teeth from full contact of more than twice the thickness of the aligner. In other words, the aligner orthodontic treatment treats the bite, but the teeth can’t fully bite except when eating. This is a contradiction. We report a case of a patient with a condition thought to be cased by this contradiction.
Ⅱ.Present Findings(At the first visit, Fig 1)
Age at first visit: 32years 2months
Gender: Female
Chief complaint: I am in the process of orthodontic treatment by a mouthpiece at a dental clinic in Tokyo. My back teeth did not mesh for more than a year. I’m worried because I show no signs of improvement. When opening mouth, I have pain in my left temporomandibular joint.
History of hearing from patients: Orthodontic treatment using Invisaline was started to treat the crowded dental arch in the clinic of the former doctor. About 1 year after the start of the treatment, she could not chew with her molars. As a result, it became difficult to eat. In addition, temporomandibular joint pain developed. When she consulted with her doctor, it was explained that her back teeth would bite once the treatment entered the final stage. Two years after the start of the treatment, she consulted with her doctor again. The dentist instructed her to wear a mouthpiece with the molars cut off. At that time, she questioned the dentist as follows. If she wears a mouthpiece with the molars cut off, it may not be the treatment results created by computer simulation at first. She couldn’t get a clear answer from the dentist, so she felt distrustful. After that, she visited our office for a second opinion.
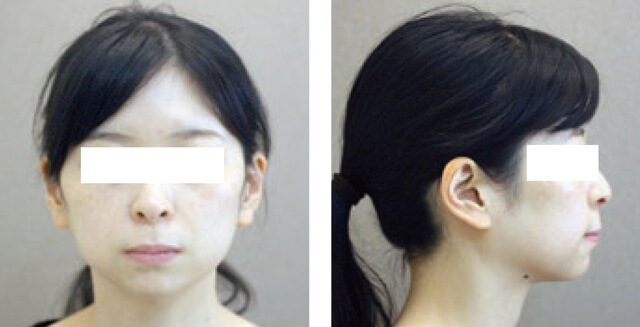
Facial findings: The patient’s face was symmetrical and slightly long. The profile was a convex type. When the lips closed, the upper and lower lips protruded 1-2 mm from the E-line.
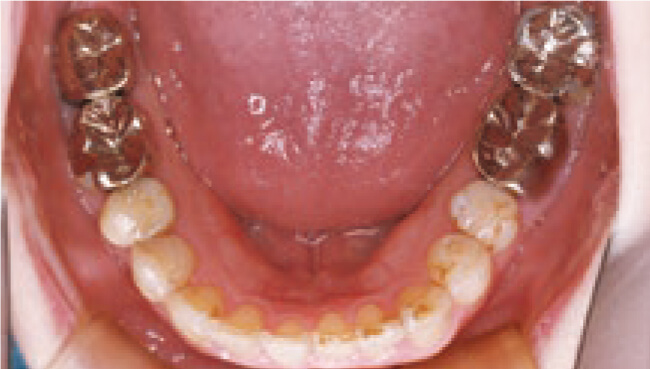
Intraoral findings: On both sides, the second premolar, first molar, and second molar had open bite. No crowded dental arch was observed.
Lateral cephalogram findings: The ANB was 5°, the maxilla was located anterior to the position of the mandible. Although the molar had an open bite, it could not be seen because of the opaque image of the prosthesis.
Panoramic x-ray photography findings: Maxillary left incisor and maxillary left second premolar were root canal treated teeth. The upper bilateral first molars were mesially inclined.





Facial and oral photo
The relationship between molars and canines was slightly Class II.
Overjet 3.5mm, Overbite3.0mm
Bilateral second premolar, first molar, second molar had open bite

Panoramic radiograph
Upper bilateral first molars were mesially inclined.

Lateral cephalogram
There was a lingual inclination of the upper anterior teeth and a labial inclination of the lower anterior teeth. An open bite of the molar could not be confirmed due to the prosthesis of the molar.
Figure 1:At first visit. <32 years and 2 months old>
Ⅲ.Reference materials (At the start of treatment at the previous doctor. Figure 2)
Age: 29years 6months
Facial findings: The face was symmetrical. There is a slight protrusion of the upper and lower lips.
Intraoral findings: Both molars and canines have Class I relationships, and good interdigitation was observed. The right first premolar had a cross bite. Crowding was observed in the lower anterior teeth.
Lateral cephalogram findings: The ANB was 4°, the maxilla was located anterior to the position of the mandible. Although the molar had an open bite, it could not be seen because of the opaque image of the prosthesis.
Panoramic x-ray photography findings: No abnormal findings were observed.





Facial and oral photo
A class I cusp fit was observed. Crowding was observed in the lower anterior teeth.
The right first premolar had a baccal cross bite.

Panoramic radiograph

Lateral cephalogram
Figure 2:Reference materials (At the start of treatment at the previous doctor.) <29years and 6 months old>
Ⅳ.Findings of superimposition of lateral cephalogram. (Fig 3)
Prior to diagnosis, the cephalograms were superimposed at the time of prior treatment by the previous doctor(blue line) and at the time of the first visit to this hospital(black line). The maxillary anterior teeth are slightly elongating and tipped towards the palatal side.

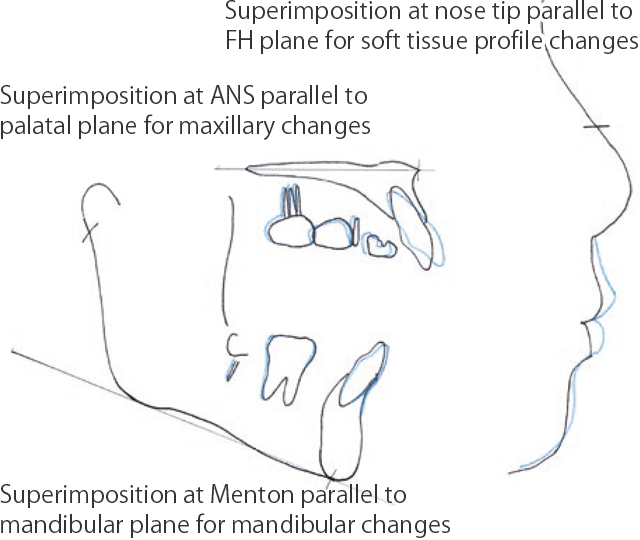
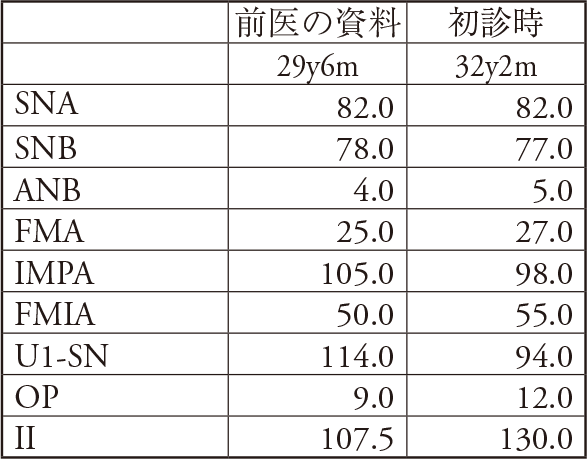
Figure 3:Superimposition of the lateral cephalogram before the start of treatment at the previous doctor (blue) and at the first visit to this hospital (black).
The maxillary anterior teeth were slightly elongating and tipped towards the palatal side. However, because the upper and lower anterior teeth were not sufficiently depressed, the mandible rotated clockwise and the molars became open bite. The lower anterior teeth were tilted labially.
Ⅴ.Diagnosis
This case was diagnosed as a molar open bite caused by the clockwise rotation of the mandible due to excessive lingual inclination of the maxillary anterior teeth.
I guess that former doctor thought the lateral expansion of the dental arch provides space for retracting upper and lower incisors. In the oral photograph, the arch width of the maxillary first molar was expanded by 3mm.
Ⅵ.Treatment plan
Attach the multi bracket device to the upper and lower jaws.Sufficient crown labial torque while tilting labial side.Rotate the mandible counterclockwise to position the original mandible. Back into place to improve open bite of the molars.I informed the patient about the treatment procedure. I also presented the patient with an option to reduce the feeling of protrusion of the upper and lower lips, which would involve the premolar extraction of 4teeth. Patient did not want the treatment involving extracting teeth, therefore, the treatment without tooth extraction was selected.
Ⅶ.Treatment progress
Standard edgewise devices(.018″ × .025″ )were attached to the upper and lower jaws. Leveling with round wire was done for 3 months. After that, bands were attached to the upper and lower second molars which made them aligned. After that, the upper and lower jaws were fitted with an ideal arch for a duration of 5 months. Up-and-down elastic was used for 5 months during treatment.
Ⅷ.Treatment result (Figure 4)
Treatment period: 10.5 months
Age at end of treatment: 33 years 2 months
Facial findings: There is no change in facial appearance compared to the initial appearance.The slight protrusion of the upper and lower lips remains.
Intraoral findings: Open bite of the molars has been treated. The midlines of the upper and lower jaws coincide. Due to the tooth size, the cusp fitting leans slightly towards class II.
Lateral cephalogram findings: FMA is reduced by 2°. ANB is reduced by 1°. UI-SN is 117°, increasing by 23°, The upper anterior teeth were tilted labially.
Panoramic radiographic findings: The parallelism of the roots was good.






Facial and oral photo
The open bite of the molars improved. The molars relationship was slightly class II, because of tooth size discordance.
The maxilla was held by a Beg type retainer and the mandible was held by a fixed retainer.

Panoramic radiograph
The mesial inclination of the upper first molar was improved

Lateral cephalogram
Figure 4:At the end of active treatment. <33 years and 2 months, active treatment period 10.5 months>
Ⅸ.Findings of superimposition of lateral cephalogram before and after treatment
The upper anterior tooth crown moves to the labial side with a slight depression. Maxillary anterior teeth roots are moving to the palate side.
The lower anterior tooth are labially inclined, but the position of the incision remains unchanged. With these changes, the mandible rotated counterclockwise, which improved the open bite of molars. The molar axis was upright. The width of the molar was reduced. Since the mandibular rotated counterclockwise, the lower facial height became slightly shorter. The upper lip protruded only slightly after treatment.
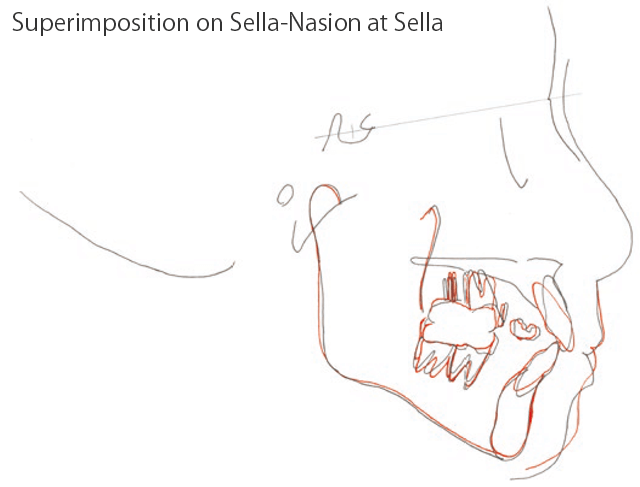
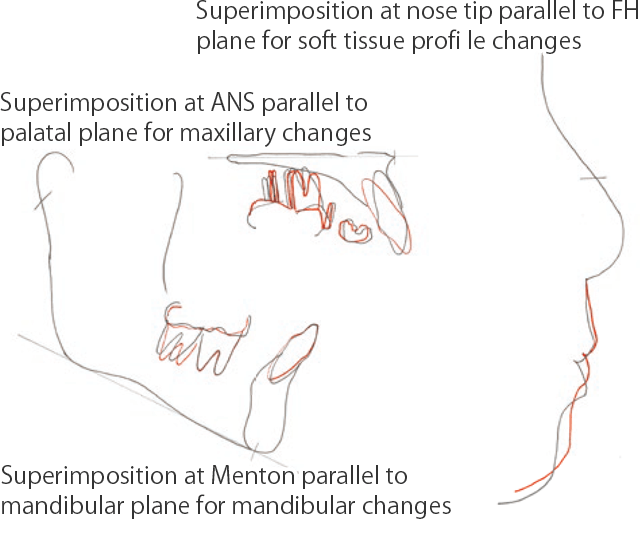
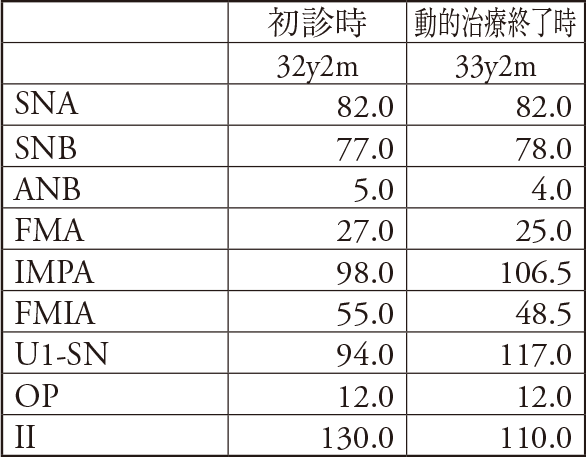
Figure 5:Superimposition of lateral cephalograms before and after treatment
The crown of the upper anterior tooth is moved to the labial side while being depressed. The upper anterior teeth roots have moved to the palate side. As a result, the mandible rotated counterclockwise and the molar openbite were improved. The axis of the molars was upwritten and the width of the molars was reduced to the original width.
Ⅹ.Discussion and conclusion
Orthodontic treatment using a mouthpiece has a contradiction that upper and lower teeth never contact when a device is attached, despite being treated for occlusion. We have presented one such case that is thought to have occured due to this contradiction. Since this one case may be a unique phenomenon, it is not possible to generalize the proposition that ” Molar open bite occlusion may occur in Orthodontic treatment using a mouthpiece “.
In actual orthodontic treatment, we often experience that the lower jaw rotates clockwise with the rotation of the occlusal plane as in the case shown here. The lower jaw rarely rotates counterclockwise. If the lower jaw rotates clockwise, the class II relationship of molars becomes stronger. If rotated in the opposite direction, class II approaches class I 3). However, the relationship between the upper jaw and the lower jaw does not change when making a treatment plan using simulation software for invisaline treatment. Changes that may occur in the body, such as rotation of the lower jaw, are not reflected in the treatment plan. In the future, more predictable diagnostic software that takes these into the account may be supplied, but it is not yet present.
Recognizing the possibility of molar open bite after treatment when selecting orthodontic treatment using a mouthpiece, informing the patient of this, and preparing a solution when it occurs before starting treatment would be beneficial.
References
1)M Zheng, R Liu, Z Ni and Z Yu: Efficiency,effectiveness and treatment stability of clear aligners: A systematic review and meta-analysis: Orthod Craniofac Res.2017 Aug;20(3):127-133.
2)Jiafeng Gu, Jack Shengyu Tang, Brennan Skulski, et al:Evaluation of Invisalign treatment effectiveness and efficiency compared with conventional fixed appliances using the Peer Assessment Rating Index: Am J Orthod Dentofacial Orthop. 2017 Feb;151(2):259-266.
3)Funio Yogosawa:Edgewise System Vol.I, Praxis art,Quintessence Publishing,Tokyo,2001.
症例情報
【主訴】マウスピースにて矯正中(他院)だが、奥歯が噛み合わない
【診断名】両側臼歯部の開咬合
【年齢】32歳2か月
【治療に用いた主な装置】マルチブラケット装置
【抜歯部位】なし
【治療期間】1年 また、治療期間と同程度の保定期間を要する
【通院回数】治療期間は12回(月に1回程度)の通院、保定期間は3回(4か月に1回程度)の通院
【治療費概算(自費)】約85万円 ※別途、初診相談料5,500円(税込)、検査診断料55,000円(税込)
【リスク 副作用】
初めて装置を装着した時やワイヤー調整後は、噛むと痛みを感じたり、違和感を持つ場合があります。
矯正治療中は歯磨きしにくい部分ができるため、むし歯や歯周病になるリスクが高くなります。
歯を動かす際に、歯根吸収や歯肉退縮が起こる場合があります。
歯並びを整え、咬み合わせを改善するため、やむを得ず健康な歯を抜くことがあります。
リテーナー(保定装置)を使わずに放っておくと、治療前の状態に後戻りすることがあります。
※ 矯正歯科治療は公的健康保険の対象外の自由(自費)診療となります。
※ 治療費用は改定していますので、現在の費用は料金ページをご覧ください。